

The choroid plexus (ChP): hydrodynamic bottleneck and ground zero for Alzheimer’s disease https://ejournals.uni-muenster.de/fnp/article/view/9368/9664
The Institute has advanced a Dual Sequestration Hypothesis (DSH) related to the protein signatures prevalent in Alzheimer’s disease. If the DSH is correct, the ChP should enlarge and become the sentinel hydrodynamic bottleneck as synthetic particles and their protein sequestrants accumulate. This terminal bottleneck or anatomical ground zero sets the stage for the DSH and systemic failure. Without ChP enlargement as the ultimate focal area for sequestration deposits, the glymphatic spread remains an unbounded process without a clear pathology. Conversely, if modern medicine cannot solve the sequestration and clogging problem at the ChP, then upstream treatments targeting the parenchyma will yield little or no clinical benefit.
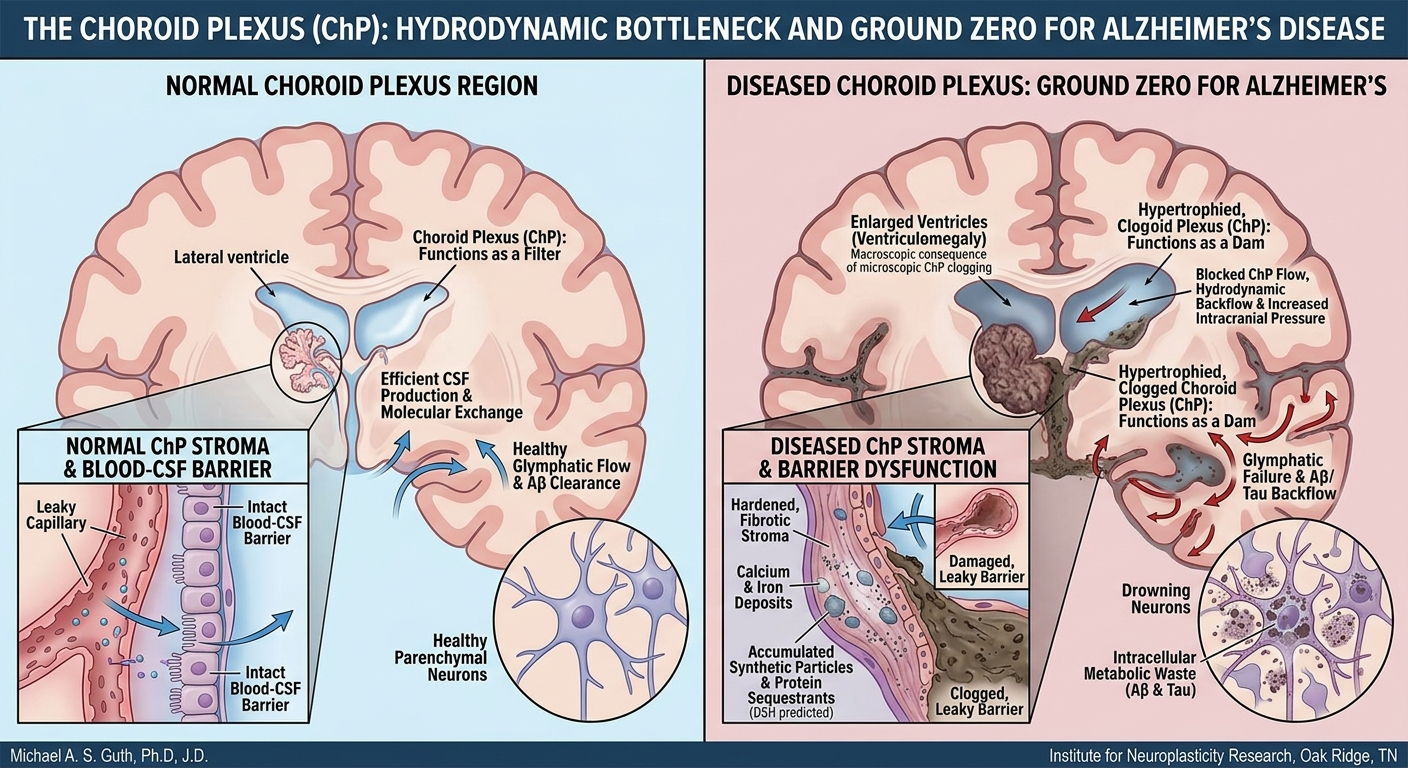
The ChP stroma supports fenestrated (leaky) capillaries, distinct from the tight BBB, enabling molecular exchange between blood and CSF and transporting immune cells into the ventricles. With aging, the stroma can become hardened and fibrotic, accumulate calcium and iron deposits, and now the DSH predicts NP deposits as well. Non-degradable particles serve as a scaffold for age-related stromal hardening, thereby turning the ChP from a filter into a dam. When the ChP becomes a dam, upstream pressure—manifesting as increased intracranial pressure or glymphatic backflow—eventually overwhelms and kills the neurons. If the glymphatic backflow stops, the metabolic waste like Aβ and Tau remains inside the individual neurons, and they drown in their own metabolic waste. By integrating the enlarged ChP as a hydrodynamic sump, the DSH becomes a closed-loop system: trigger sequestration → lytic release → ChP clogging and enlargement.
An enlarged or hypertrophied ChP can overproduce CSF or physically obstruct its flow and thus cause the brain’s ventricles to become enlarged or dilated (ventriculomegaly). Enlarged ventricles in the brain are a well-known hallmark of AD, yet their cause has remained mechanistically unexplained. The DSH provides that missing link: ventriculomegaly is the macroscopic consequence of microscopic clogging at the ChP.
Recent findings by Pang et al. (2026) provide clinical support for the DSH. They found that MRI scans of patients suffering from long COVID displayed enlarged ChP and reduced cerebral blood flow, which are both associated with AD-like dementia. Long COVID brain fog is an acute manifestation of the same sequestration phenomenon. The DSH is the unifying framework for both post-infectious (COVID) and environmental (NP) neurodegenerative risk. The clinicopathological cascade begins with ChP immune surveillance, followed by non-degradable particle trapping, barrier dysfunction, and glymphatic failure: a sequence now visible on medical imaging and traceable back to its molecular origins. At the ChP, viral or environmental toxicology crashes into clinical neurology.
The DSH defines the ChP as both the final stage of the accumulation and the starting point of the permanent dementia-like decline. With clinical urgency, the MRI findings of ChP enlargement are the definitive signal that the ground zero event is occurring in the patient. The ChP is where the sequestration cycle reaches critical mass, triggering the glymphatic failure that characterizes the transition from acute brain fog to chronic neurodegeneration. If the ChP is ground zero for the collapse, then a therapy targeting clearance of the ChP becomes the logical cure for this form of neurodegeneration.
 Posted in
Posted in