Dear Drs. xxxxxxxxxxxx and xxxxxxxxxxxxxxx,
I write to inquire whether the Journal of Clinical Epidemiology would consider a Perspective manuscript entitled xxxxxxxxxxxxxxxxxxxxxxxx.
The manuscript (~5,100 words, 37 references) addresses a problem that experienced clinical epidemiologists and HTA reviewers recognize but that the published literature has been reluctant to name directly: when Phase 3 trials produce overall survival benefits measured in weeks to a few months — statistically significant, clinically marginal — the center of gravity in value assessment shifts to forward-looking economic models that extrapolate survival curves decades beyond the observed trial window. At that horizon, the distinction between a conservative, empirically grounded projection and a flagrantly optimistic one is not self-evident from the model output. Both can be produced using individually defensible methods. Both will pass peer review. Only one approach will be systematically favored by the pharmaceutical sponsors preparing regulatory submissions.
This manuscript identifies where that asymmetry lives. It reverse-engineers five core analytical domains — parametric survival extrapolation, partitioned survival model construction, Markov state transition engineering, utility and QALY construction, and healthcare resource utilization modeling — and in each case distinguishes the conservative, realistic application from the optimistic, advocacy-oriented one. The analysis is not a theoretical taxonomy. It uses worked numerical examples and recent Phase 3 trial data across four tumor types to show concretely how selection among statistically equivalent model specifications produces lifetime survival estimates that diverge by years, and how those divergences compound across domains into cost-effectiveness conclusions that bear little resemblance to what the trial actually demonstrated.
The argument is structural, not accusatory. This is not an allegation of fraud or bad faith, and the manuscript does not contest the clinical efficacy of any compound discussed. The claim is that the dossier production process contains well-defined leverage points that systematically favor optimistic extrapolation, that these leverage points are individually defensible and collectively distorting, and that HTA bodies and payers currently lack the auditing vocabulary to identify them reliably. The manuscript closes with four low-cost, implementable transparency reforms — pre-specified survival model selection criteria, independent extrapolation, OS maturity thresholds before PFS-based models are accepted for formulary decisions, and mandatory disclosure of all fitted parametric specifications — that address the problem without imputing misconduct.
The author is an independent scholar and Director of Health Outcomes Research and Causal Evidence at the Institute for Neuroplasticity Research in Oak Ridge, Tennessee, with direct prior experience in pharmaceutical HEOR and survival analysis across hematologic oncology and solid tumor treatment compounds at major biopharma firms and smaller start-ups. He has no current financial relationship with any pharmaceutical firm or ongoing oncology trial. That independence is material: the manuscript carries no industry sponsorship or trial affiliation, and its argument does not need to accommodate any sponsor’s dossier interests. The Journal of Clinical Epidemiology is one of the few venues whose editorial tradition — including its sustained engagement with surrogate endpoint validity, research bias, and the translation of trial evidence into policy — makes it the right home for this article.
I would be pleased to submit the full manuscript for your consideration as a Perspective.
Thank you for your time.
Michael A. S. Guth
Michael A. S. Guth, Ph.D., J.D.
Director, Health Outcomes Research & Causal Evidence
Institute for Neuroplasticity Research
[email protected] | (865) 483-8309 www.linkedin.com/in/populationhealthmanagement
“Pioneering spirit should continue, not to conquer the planet or space, but rather to improve the quality of life.” — Bertrand Piccard
Clinical Evidence Generation & Publications Track Record:


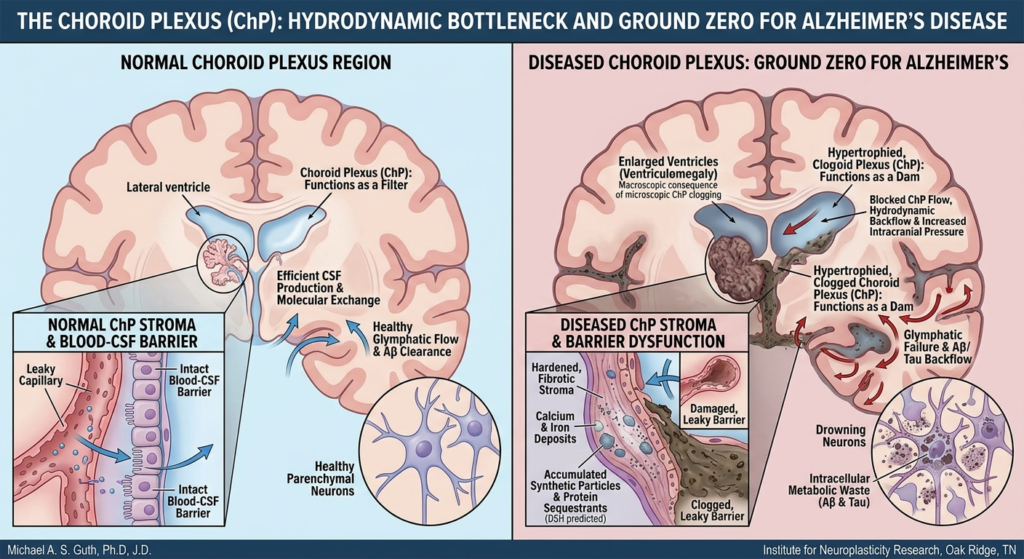








𝐍𝐞𝐰 𝐏𝐮𝐛𝐥𝐢𝐜𝐚𝐭𝐢𝐨𝐧 𝐢𝐧 𝐅𝐫𝐞𝐞 𝐍𝐞𝐮𝐫𝐨𝐩𝐚𝐭𝐡𝐨𝐥𝐨𝐠𝐲 (𝐉𝐮𝐧𝐞 𝟐𝟎𝟐𝟔) 𝐈 𝐚𝐦 𝐩𝐥𝐞𝐚𝐬𝐞𝐝 𝐭𝐨 𝐬𝐡𝐚𝐫𝐞 𝐨𝐮𝐫 𝐥𝐚𝐭𝐞𝐬𝐭 𝐜𝐥𝐢𝐧𝐢𝐜𝐨𝐩𝐚𝐭𝐡𝐨𝐥𝐨𝐠𝐢𝐜𝐚𝐥 𝐮𝐩𝐝𝐚𝐭𝐞 𝐚𝐝𝐝𝐫𝐞𝐬𝐬𝐢𝐧𝐠 𝐚 𝐩𝐞𝐫𝐬𝐢𝐬𝐭𝐞𝐧𝐭 𝐩𝐚𝐫𝐚𝐝𝐨𝐱 𝐢𝐧 𝐀𝐥𝐳𝐡𝐞𝐢𝐦𝐞𝐫’𝐬 𝐝𝐢𝐬𝐞𝐚𝐬𝐞: 𝐰𝐡𝐲 𝐭𝐡𝐞𝐫𝐚𝐩𝐢𝐞𝐬 𝐭𝐚𝐫𝐠𝐞𝐭𝐢𝐧𝐠 𝐭𝐡𝐞 𝐫𝐞𝐦𝐨𝐯𝐚𝐥 𝐨𝐟 𝐚𝐦𝐲𝐥𝐨𝐢𝐝-β 𝐩𝐥𝐚𝐪𝐮𝐞𝐬 𝐚𝐧𝐝 𝐭𝐚𝐮 𝐭𝐚𝐧𝐠𝐥𝐞𝐬 𝐜𝐨𝐧𝐬𝐢𝐬𝐭𝐞𝐧𝐭𝐥𝐲 𝐬𝐡𝐨𝐰 𝐚 𝐜𝐫𝐢𝐭𝐢𝐜𝐚𝐥 𝐝𝐢𝐬𝐬𝐨𝐜𝐢𝐚𝐭𝐢𝐨𝐧 𝐟𝐫𝐨𝐦 𝐜𝐨𝐫𝐞 𝐜𝐥𝐢𝐧𝐢𝐜𝐚𝐥 𝐩𝐚𝐭𝐡𝐨𝐠𝐞𝐧𝐞𝐬𝐢𝐬.
𝐈𝐧 “𝐀𝐥𝐳𝐡𝐞𝐢𝐦𝐞𝐫’𝐬 𝐝𝐢𝐬𝐞𝐚𝐬𝐞 𝐢𝐧 𝐭𝐡𝐞 𝐏𝐥𝐚𝐬𝐭𝐢𝐜𝐞𝐧𝐞 𝐞𝐫𝐚: 𝐚 𝐜𝐥𝐢𝐧𝐢𝐜𝐨𝐩𝐚𝐭𝐡𝐨𝐥𝐨𝐠𝐢𝐜𝐚𝐥 𝐮𝐩𝐝𝐚𝐭𝐞 𝐨𝐧 𝐭𝐡𝐞 𝐝𝐮𝐚𝐥 𝐬𝐞𝐪𝐮𝐞𝐬𝐭𝐫𝐚𝐭𝐢𝐨𝐧 𝐨𝐟 𝐚𝐦𝐲𝐥𝐨𝐢𝐝 𝐚𝐧𝐝 𝐭𝐚𝐮 𝐚𝐬 𝐡𝐢𝐣𝐚𝐜𝐤𝐞𝐝 𝐢𝐧𝐧𝐚𝐭𝐞 𝐢𝐦𝐦𝐮𝐧𝐞 𝐫𝐞𝐬𝐩𝐨𝐧𝐬𝐞𝐬,” 𝐰𝐞 𝐩𝐫𝐨𝐩𝐨𝐬𝐞 𝐭𝐡𝐞 𝐃𝐮𝐚𝐥 𝐒𝐞𝐪𝐮𝐞𝐬𝐭𝐫𝐚𝐭𝐢𝐨𝐧 𝐇𝐲𝐩𝐨𝐭𝐡𝐞𝐬𝐢𝐬 (𝐃𝐒𝐇).
Key Frameworks Addressed:
The Sequestration Response: Reinterpreting Aβ and tau as conserved, compartment-specific innate immune barriers—an extracellular “sarcophagus” and an intracellular “lockbox.”
The Synthetic Trigger: How pervasive, indestructible environmental nanoplastics (NPs) act as permanent nucleation seeds, hijacking these responses into an indigestible synthetic protein complex.
Immune Frustration & Progression: Chronic microglial engagement triggers NLRP3 inflammasome activation, leading to pyroptotic cell death. This lytic release distributes intact synthetic seeds via glymphatic flow, physically obstructing clearance and driving Braak stage progression.
Therapeutic Relevance:
The DSH offers a structural explanation for the therapeutic failure of anti-Aβ/anti-tau antibodies (removing the biological barrier but leaving the synthetic core) and frames amyloid-related imaging abnormalities (ARIA) as an inflammatory rebound.
The paper calls for a necessary paradigm shift in neuropathological practice—specifically, utilizing novel detection techniques to visualize the predicted synthetic NP cores within classical lesions.
Full text and citation details below:
Journal: Free Neuropathol. 2026 Jun 22;7:14.
DOI: 10.17879/freeneuropathology-2026-9368
PMID: 42344202
hashtag#AlzheimersDisease hashtag#Neuropathology hashtag#Neuroinflammation hashtag#EnvironmentalToxicology hashtag#Biopharma hashtag#RWE